Dry Fasting Improves Fertility in Both Men and Women (in moderation)
By Yannick Wolfe
Dry fasting, which involves abstaining from both food and water for short periods, is emerging as a potential tool for enhancing fertility in both sexes. While research is still developing, evidence suggests it can positively influence hormone levels, particularly for those with infertility linked to metabolic issues like obesity, insulin resistance, polycystic ovary syndrome (PCOS) in women, or hypogonadism in men. By resetting the endocrine system and boosting insulin sensitivity during refeeding, dry fasting may offer a net benefit.
💡I have seen many cases of improved fertility following a 5 day dry fast. I would advise against continual fasting to try to achieve it though, as after a certain amount of fasting, the negatives start to outweigh the positives. Think of it like a hill. You want to climb it just enough, because once you start overshooting it, you're heading back down.
Keep in mind that fasting itself is a low-energy state that can slow things down, including sperm motility. Still, the magic lies in the refeed and subsequent hormone normalization, and FH and testosterone boost.
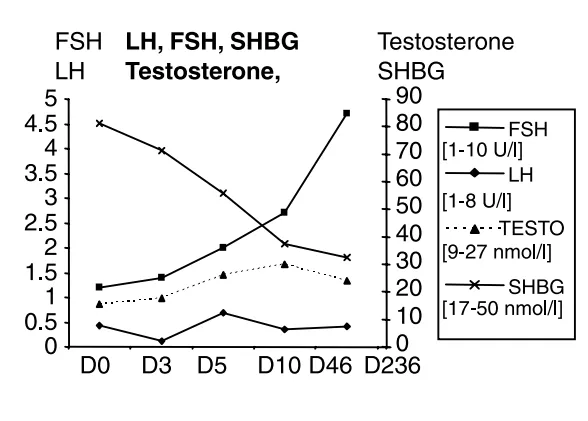
LH, FSH, SHBG, and Testosterone levels during refeeding after a fast
refeeding period and hormone levels after a 44 day water fast
These hormonal shifts promote fertility restoration: restored follicle-stimulating hormone (FSH) and testosterone levels can boost sperm production and motility in men, while lower sex hormone-binding globulin (SHBG) and dehydroepiandrosterone sulfate (DHEAS) enhance free hormone availability and reduce androgen excess, a common issue in PCOS.
Studies on related practices like intermittent or Ramadan fasting highlight improvements in women's reproductive health, including better menstrual regularity, reduced androgens (such as a 9% testosterone drop in PCOS cases), and enhanced ovulation.
However, risks include temporary hormone disruption during the fast (e.g., suppressed FSH and testosterone), so benefits typically emerge post-refeeding.
This is why you will keep on hearing that the magic of the fast is in the refeed. You need to nurture the body after the fast by giving it tons of fuel and energy for restoration depending on where you are in your health journey. If you're early in it and not fighting symptoms of fatigue, you can refeed ketogenically, but otherwise you will need to fuel with much more carbohydrates to get all the benefits of the stem cells and insulin sensitivity long term.
You have been told type 2 diabetes is chronic and only worsens, that fasting can reverse it, and that fasting is dangerous for diabetics. They cannot all be true. Here is the honest version: what the reversal evidence really shows, the four-tier safety line set by your medications, why a dry fast removes your ability to treat a low, and how to break a fast without spiking. The reversal is real, but it is a supervised, water-before-dry move, not a license to change your meds.
You take something every day, and nobody told you whether to keep taking it through a fast or stop it. Both choices can hurt you. Here is the honest map: the drugs that get dangerous when you are dehydrated, the one class you must never pause, the medications that are actually fine to time around a fast, and the five-minute prep that turns "talk to your doctor" into a useful conversation instead of a shrug.
You read that fasting is one of the most powerful things you can do for your health, so you did what the guys do, fasted often and pushed the windows, and your period got weird and your energy tanked. You were not doing it wrong so much as doing it like a man. Here is what is actually different for a woman's body, the timing that makes dry fasting work with your hormones instead of against them, and why the metabolic layers matter even more for you.